Maybe you just got back the results of a neuropsych evaluation for your child, or the school’s evaluation. Or, it was one specialist after another like a trail of breadcrumbs as you unraveled the clues: the pediatrician diagnosed the ADHD; the developmental pediatrician noticed the core weakness and symptoms of tracking problems leading to recommendations of OT and vision evaluations. The OT eval revealed sensory processing struggles and also recommended you find a child therapist to help support dysregulation. The vision evaluation revealed the possibility of dyslexia in addition to recommending therapy for tracking and convergence insufficiency…
Suddenly, you’ve got quite a task list and it may feel like a race against time to get your child everything they need to thrive (or survive). Everyone talks about how “early intervention is critical.” And it is important. How do you wait on the vision therapy if you want your child to read? How can you put off the therapist when your child is struggling with big feelings at home and at school? Obviously, they need the occupational therapy so that they can learn to grip a pencil properly and sit at a desk.
How can you care about a budget when this is your child and they need all these therapies and interventions, NOW?!
And like that, *snap,* the race is on. All of it is important. Urgent. Expensive. Time consuming. Vision therapy Thursdays. OT Fridays. Therapist on Mondays. Dyslexia tutor 2x a week, and some people are telling me that is not enough time to make significant progress with my child’s dyslexia. Then, auditory processing comes up and the recommendations come rolling in. OT leads to speech, which leads to mayofascial therapy. And that is just Sally, and she has siblings with their own needs. Many times with neurodivergence, we make continual discoveries. There isn’t just one single and simple diagnosis, but over time like peeling an onion we discover more layers to these amazing kids.
If some version of this sounds familiar, take a breath. Know that you’re an AMAZING PARENT. I don’t say that lightly. I am shouting it from my core to you. You’re utterly amazing. You’re not failing your child.
But the question stands: how do we manage this? And fully, the answer is that you don’t. Believe me. I’ve tried. Even if you have the money and the time, even if your kid homeschools and has a flexible schedule, your child can only manage so much intervention before they burn out and intervention loses effectiveness. So take a few bricks off the load you are carrying and take another deep breath. You’ve got this. It’s also paramount that you do what you are truly capable of and not more. If you’re maxed out and trying to push forward, the kids sense that stressed energy. They need you to be healthy and operating within your capacity.
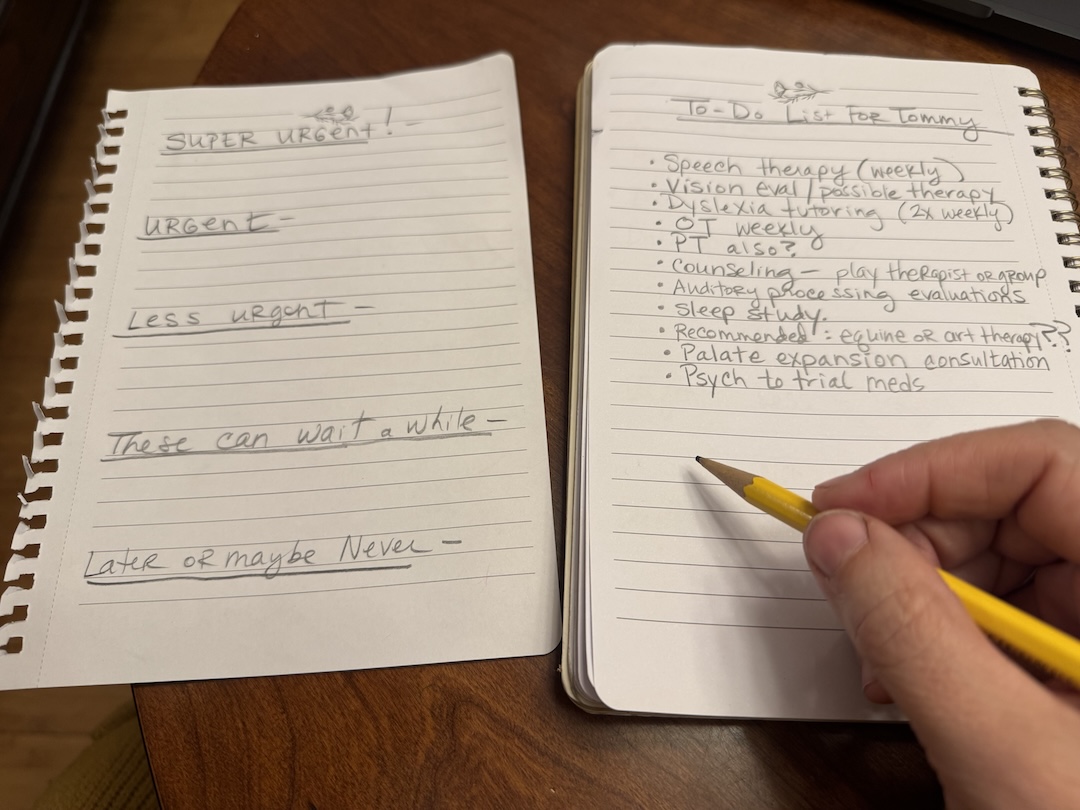
Start by creating a triage. In this situation, by triage I mean that you are going to sort through and figure out the urgency level of needs. I suggest you decide which interventions to prioritize, which to wait on, and which to possibly place in the pile of things that you may get to or might actually never do at all. Once you have that triage plan, it’s okay to change your mind and tweak your intervention list. You can change your plan at any time. Quit OT and switch the tutor out. Nothing is set in stone. You’re the expert on your child, and that matters. With therapy order, sometimes one therapy is more effective if done AFTER a particular therapy. For instance, if your child needs both OT and vision therapy, there are benefits to doing OT first and then following it with the vision therapy. All that vision work relies on the foundation of a strong core. So, instead of feeling guilt about not getting them both done at once, there may be benefits to doing OT and then vision therapy. And that gives you more bandwidth and is easier on the budget, for sure! Another example could be speech therapy and mayofascial therapy to help the tongue to be more independent from the lower jaw. My son was in speech when we learned he needed mayofascial therapy. Rather than layering one on top of the other, we paused regular speech until the season of mayofascial therapy was over. And, mayofascial still allowed him to make strides in articulation.

Consider what to table or cross off the list altogether. We tabled for a few years going out of state for a specific evaluation. And then, when we did it, we arranged for four of us to all be evaluated. So, we waited until it was the right timing and we were ready with the budget, and then we made it really worth our while by evaluating the whole family at once. There are some other treatments that we decided were too time-consuming, stressful, expensive, and didn’t offer enough value. Also, there are other therapies that weren’t right for our family. That is something for you to research and get second opinions on, to make sure that a therapy is the right fit for your child. With that in mind, you can also take some time to make sure you’ve found the right specialist to work with your child. Sometimes we stayed with a specialist for a while but it didn’t feel like a good fit, and I learned my gut was right. Listen to your gut on that and don’t feel stuck. Even when someone is the “only” specialist for a therapy in your area, it may be you take a pause. I replaced a poor-fit therapy at one point with a specialist who was online, and it was fabulous. I promise, we accomplished 5x as much. My gut was right.
Find your core team and lean in on them for guidance. What I discovered is that there are some specialists who are really part of my child’s team. And then there are others who are not so much. When you take in advice, make sure it is from people that you’ve vetted and truly trust. If someone gives you an uneasy feeling, pause before considering them to be members of that core team of trust. Over time my team has shrunk and grown. I share more about finding the right specialists here.
Cheaper by the Dozen, so to speak. Other ways to simplify when you have multiple kids could mean coordinating a therapy that two need so that they get it done at the same time. For instance, I took two of my kids to OT together. Two birds with one stone. We also paired two kids together for mayofascial therapy. In that situation, we were able to place them in one session with a provider together and that meant a significant discount in cost, in addition to the time saver. We even coordinated surgery (related to airway issues) for two kids having outpatient surgery at the same time. Since biological siblings share a lot of hereditary features, you may find like we did that siblings need some of the same intervention supports.
Heavily prioritize and protect space for whatever it is that your child loves. This is the activity that makes their face light up- the type of thing they’d wake up early on a Saturday to do. Soccer? Art? Theater? Bird watching? Video gaming? (you could join in and have family tournaments?) The interventions are important, but that isn’t where your child thrives, finds their joy, and comes to life. In fact, some interventions are downright hard, draining and exhausting. Don’t replace the thing that lights up their soul for a deficits-focused intervention. The experts at Uniquely Bright Life, an organization that supports twice exceptional families, recommends focusing time and energy on strengths over deficits in a 2:1 ratio as a good rule of thumb. This builds a reserve of strength and self-efficacy that will help fuel them through the hard things.
Carve out space. Now that you’ve picked a couple therapies to start, consider how to make space for them. Your child may not have the capacity to just add those in on top of all the other demands and loads they carry. Are they school age? Do they have homework? Are they sitting at a desk all day dealing with loud noises, crowded classrooms and fluorescent lights? For many children, seven hours in a traditional classroom is fully depleting and they come home drained. Can any interventions happen during the school day? (but, make sure the child isn’t pulled from their favorite class.) For my kindergartner, I let the school know I’d pick him up early two days a week for private OT and speech. This was easier to do because he was in private school at the time. If you try for this, it is typically easier to pull them at the end of the day than to bring them late. Attendance is taken in the morning and for public school, that attendance means tax dollars for the school. They need you there in the morning so they get paid.
Clearing space for more demands could also mean cutting out some of the other ongoing demands for a while. Remember, you’re in a triage state. It’s ok to give your child room to breathe and have fun. For instance, when my son was doing vision therapy, which is exhausting and difficult work, we counted it in the space of household chores. He’d still throw his own laundry in the basket, but I wasn’t asking him to do any extras. Vision therapy was “extra” enough. While we mostly avoid extrinsic rewards, vision therapy is one intervention where we offered incentives. It was just a lot to ask a kid to do. Really hard interventions in our family means we lower the homework expectation for an elementary-aged kid. If they’re in school, then you’ll need to work this out with the administration. There might be some push-back but it’s elementary school- It’s a reasonable accommodation. Make certain it’s in writing. Kids must have a chance to play.
Whatever you decide, don’t forget that you’re the expert on your kiddo. You can change your mind. You can quit or pause a therapy. You can switch therapists. You can add a therapy. Take your time. This is a journey, not a quick sprint. Look for the light in your child’s eyes and follow that above all else.
As my mom used to say, You’ve got this!
With love,
Christina
Leave a Reply